Resident Physician Christ Hospital Marlboro, New Jersey, United States
Introduction: We present a case of a woman with an atraumatic, idiopathic subdural hematoma without predisposing factors. Over a month, she was readmitted multiple times as the subdural hematoma progressed. However, with appropriate management, outcomes were improved. We highlight the importance of developing a diagnostic and treatment approach for spontaneous idiopathic subdural hematomas, an increasingly common entity.
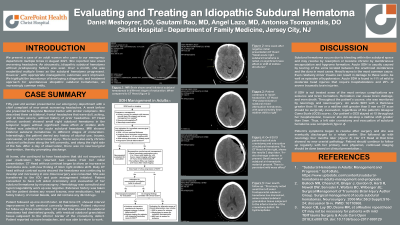
Case Study: Fifty-year-old woman presented to our emergency department with a chief complaint of new onset worsening headaches. She described them as bilateral, frontal headaches that were dull, aching, and at times severe, without history of prior headaches. CT Head without contrast showed small right subdural hematoma in the temporal region without significant mass effect or midline shift. Patient was admitted for acute subdural hematoma. MRI showed bilateral subdural hematomas in different stages of maturation. Interestingly, the patient denied any history of alcohol use, trauma, concussion, or prior intracranial injury. There were also early chronic subdural collections along the left convexity, and along the right side of the falx. After a day of observation, there was no neurosurgical intervention, thereby prompting discharge.
At home, she continued to have headaches that did not respond to pain medication. She returned two weeks from her initial presentation. CT Head without contrast began to show an increase in hematoma size, with new finding of 3mm right midline shift. Daily CT head without contrast scans showed the hematoma was continuing to develop and increasing in size. Neurosurgery was consulted. She was transferred to the ICU and pain management initiated. Patient consented to have left sided craniotomy and evacuation of her subdural hematoma by neurosurgery. Hematology was consulted and hypercoagulability work up was negative.
Patient followed up one month later. At that time CT, showed interval improvement in left cerebral convexity hematoma. Patient returned for follow up three months later, CT at that time showed the subdural hematoma had diminished greatly, with residual subdural granulation tissue subjacent to the inferior border of the craniotomy defect. Patient reported no more headaches, and was able to return to work.
Discussion: Based on osteopathic principles, we allowed time for the body to self-heal. When we saw there was danger progression of the hematoma, neurosurgical intervention was done. The patient had no risk factors, such as trauma, or hematological diseases. Her subdural expanded in a short period of time, unusual for cases with no predisposing factors. With proper intervention, her course was benign, and she improved.

 photo")